Why Prescription Drugs Cost So Much in the U.S.
From “Most Favored Nation” Pricing to Drug Patents Explained
I kept hearing the phrase “Most Favored Nation” pricing in the news and realized I had no idea what it actually meant. So I decided to do a deep dive and keep asking questions to see if I could help us all make some sense of it.
Americans pay the highest prescription drug prices in the world. For someone on Medicare, that can mean hundreds or even thousands of dollars a year out of pocket. But the reasons behind those prices are far more complicated than most headlines suggest.
If you’ve been following the news, you’ve heard a lot of noise about drug pricing. President Trump is talking about "Most Favored Nation" pricing. The Biden administration took steps to negotiate Medicare drug prices for the first time. And there's a constant, confusing debate about patents, government funding, and why your medications cost what they do.
It’s easy to get lost in the jargon. But for Mainers on Medicare, these aren't abstract policy debates—they directly impact your monthly budget and your access to the medications you need.
This post will pull back the curtain on the entire system. We'll explore the radical proposals, the moderate reforms, and everything in between, so you can understand what's at stake and how it might affect you.
Key Takeaways
• Americans pay significantly more for brand-name prescription drugs than people in other countries.
• “Most Favored Nation” pricing aims to tie U.S. drug prices to lower international prices.
• Much early drug research is funded by U.S. taxpayers through the NIH.
• The patent system encourages innovation but can also keep prices high through practices like patent “evergreening.”
• Several reforms are being debated, from international price benchmarking to major changes in the patent system.
Part 1: What Is "Most Favored Nation" Pricing?
The concept of "Most Favored Nation" (MFN) pricing sounds like international trade jargon, but at its core, it's a simple idea: The U.S. should pay the same low prices for prescription drugs that other countries pay.
How It Would Work:
The U.S. would identify a basket of similar countries (like Canada, Germany, France, and Japan).
For a given brand-name drug, the U.S. price would be benchmarked against the prices in those countries.
After adjusting for economic differences (like GDP per capita), the U.S. would set its price based on the lowest prices found abroad .
The Goal: To slash the high list prices of brand-name drugs that lack generic competition .
The Complication: Lower list prices don't always mean lower costs for you. Your copay or coinsurance is based on your insurance plan's negotiated rate. If the list price drops but your plan doesn't adjust your cost-sharing, your savings could be minimal . Furthermore, the policy faces steep legal challenges and questions about whether the administration has the authority to impose it without Congress .
Part 2: But Wait – Doesn't the Government Already Pay for These Drugs?
This is where the debate gets deeper. A crucial fact often left out of the conversation is that your tax dollars have already paid for much of the early research that leads to new drugs.
The primary agency responsible for this is the National Institutes of Health (NIH) , which funds basic scientific research at universities and institutions across the country. Consider these striking statistics:
A 2023 study found that NIH funding contributed to research associated with 99.4% of all drugs approved by the FDA between 2010 and 2019 – a total investment of $187 billion .
A 2025 study in Science concluded that a 40% cut in NIH funding would have directly impacted research associated with over half of all drugs approved after the year 2000 .
So, the public pays to discover the science, and then pays again—through high drug prices—for the finished product. This is often called the "double payment" problem, and it's a powerful argument for those who want the government to have more power to negotiate lower prices .
Part 3: The Bayh-Dole Act – How Universities Got Into the Patent Game
This brings us to a critical piece of legislation you've probably never heard of: the Bayh-Dole Act of 1980.
Before Bayh-Dole, if a university researcher made a discovery using a federal grant, the patent rights belonged to the government. And there they sat. Less than 5% of government-held patents were ever developed into actual products .
Bayh-Dole flipped the script. It allowed universities to own the patents on their federally funded discoveries and license them to private companies for development .
The Results Have Been Staggering:
Over 580,000 inventions disclosed .
More than 19,000 startups launched .
Nearly $2 trillion in economic output.
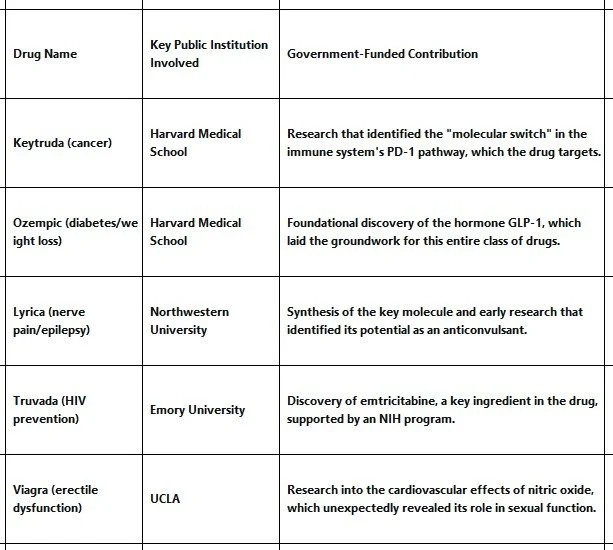
Drugs like Keytruda (cancer), Ozempic (diabetes/weight loss), and Lyrica (nerve pain) all have their roots in publicly funded university labs. Here are some others:
The Government's Safety Net: "March-In Rights"
Bayh-Dole includes a powerful provision called "march-in rights." The government retains the right to step in and license a patent to a third party if the invention is not being made available to the public on "reasonable terms." For decades, activists have argued that "reasonable terms" should include the price of a drug. If a drug developed with public money is too expensive, they say, the government should march in and let a competitor make it cheaper. This has never been done, but it remains a live legal and political debate.
Part 4: The "Where It's Made" Problem – A Tale of Two Supply Chains
Now, let's add another layer: Where are these drugs actually made?
The U.S. effectively has two separate drug supply chains, and the difference is stark.
Brand-Name Drugs (The MFN Target): These are often made in complex, resilient global supply chains. The high prices they command allow companies to invest in quality and redundancy.
Generic Drugs (The Offshoring Story): This is where "where it's made" matters most. The vast majority of generic drug ingredients come from India and China. Why? Because the generic drug market is a "race to the bottom" on price. To survive on razor-thin profit margins, manufacturers must seek the absolute cheapest production, leading them overseas.
This creates a "brittle" supply chain vulnerable to shortages and quality issues. And here's the kicker: a major RAND Corporation study found that while the U.S. pays 422% more for brand-name drugs than other countries, it pays only 67% of what other countries pay for generics. For a combined total for all drugs the U.S pays 278% of prices than other countries.
This chart breaks down the comparison for seven major countries. It clearly shows the U.S. pays a massive premium for brand-name drugs but gets a bargain on generics .
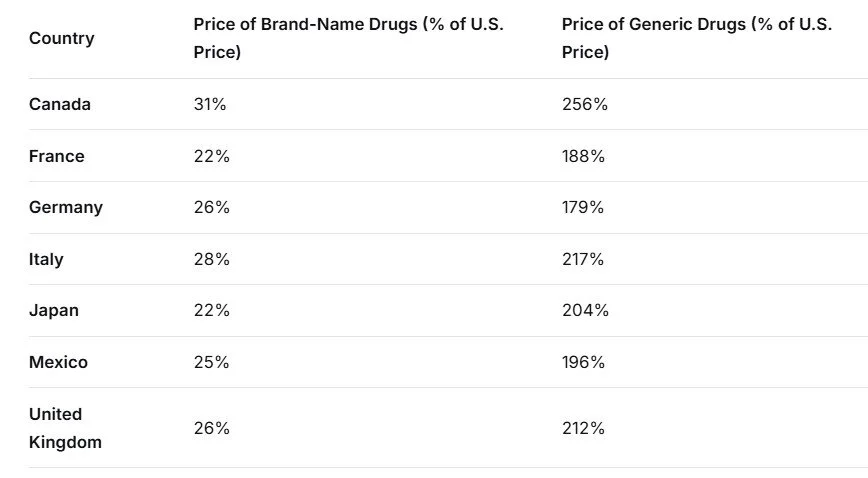
What this means: For a brand-name drug that costs $100 in the U.S., it would cost only $22 in France or Japan. However, for a generic drug that costs $100 in the U.S., it would cost $256 in Canada and $212 in the UK.
So, your tax dollars funded the research, the government created a system to commercialize it, companies offshored production to keep generic prices low, and now the U.S. wants to use other countries' low prices to bring brand-name costs down. It's a complex web.
Part 5: The Radical Solution – What If We Just Abolished Patents?
All of this leads us to the most fundamental question of all: What if we just got rid of drug patents?
This idea is being seriously proposed by academics in leading journals like The Yale Law Journal. The argument goes like this:
Patents create monopolies. Monopolies mean high prices and limited access.
The real cost isn't the molecule, it's the data. Discovering a new compound is often the result of government-funded university research. The expensive part is proving it's safe and effective through clinical trials. We don't need a patent on the molecule; we need a way to pay for the trials.
A "Prize System" Alternative: Instead of patents, the government could offer a large, one-time "prize" to any company that successfully brings a new drug to market. Once the prize is paid, the drug would be off-patent immediately, and any company could make it as a generic. This would break the link between R&D costs and monopoly prices forever.
The Counterargument:
The pharmaceutical industry argues that this would destroy innovation. They point to the "free rider" problem: other wealthy countries get low prices by threatening to exclude drugs from their national health systems. They can do this because they are effectively "free-riding" on the high prices paid in the U.S., which fund the bulk of global R&D. If the U.S. capped its prices to match theirs, global investment in new drugs would plummet.
Furthermore, developing a drug costs an average of $2.6 billion and takes 10-15 years, leaving only a few years of effective market exclusivity to recoup that investment. Without the promise of that exclusive period, no rational investor would take the risk.
Part 6: The Middle Ground – Stopping "Evergreening"
Between the status quo and full abolition lies a more targeted reform: stopping "patent evergreening."
Evergreening is the practice of piling new patents on an old drug to extend its monopoly far beyond the original 20-year term. A company might patent the original molecule, then file additional patents for a specific dosage, a new formulation, or a new method of use. This creates a "patent thicket" that is so legally complex and expensive for generic companies to challenge that they simply stay out of the market.
The impact is enormous. Look at these examples:
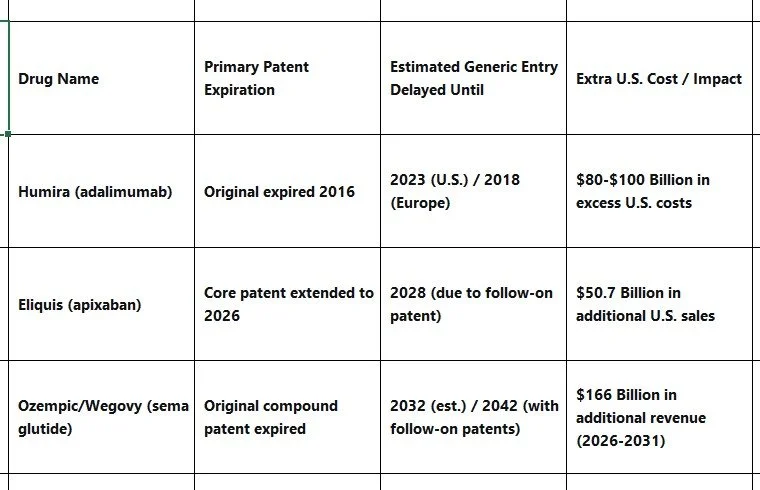
Notice that in Europe, where patent rules are stricter, Humira faced competition five years earlier.
How to Stop It:
Stricter Patentability Standards: India has a law (Section 3(d)) that prevents companies from getting a new patent on an old drug unless they can prove a significant increase in clinical efficacy. This has kept cancer and HIV drug prices 70-90% lower than in patent-protected markets.
Regulatory Exclusivity: Instead of patents, give a company a fixed, non-renewable period (e.g., 10 years) where they are the only ones allowed to market the drug based on their clinical trial data. After that, any competitor can use that data.
Using Antitrust Law: Treat patent thickets as the illegal monopolistic practices that they are.
💡 The Bottom Line for Mainers
So, where does this leave you? Educated if nothing else!
"Most Favored Nation" pricing is a direct attack on high brand-name drug prices by linking them to lower international rates. It could lower list prices, but it may not lower your out-of-pocket costs, and it faces major legal hurdles.
Your tax dollars already fund the early-stage research for most new drugs through the NIH. The Bayh-Dole Act allows universities to patent and profit from that research, creating the "double payment" problem.
Where a drug is made matters for supply security, but not for the MFN price calculation. The U.S. gets a great deal on generics (thanks to offshoring) but pays a massive premium for brand-name drugs.
Abolishing patents entirely would be a seismic shift that could make drugs incredibly cheap but might also kill the incentive for future innovation. It would require a massive, untested government funding system to replace it.
Stopping "evergreening" is a more targeted reform. By preventing companies from piling new patents on old drugs, we could ensure that when a drug's original patent runs out, prices actually fall as intended.
At www.mainelymedicarehelp.com, my goal is to help you navigate this complex landscape. Whether it's understanding your Part D coverage, comparing plans during Open Enrollment, or just making sense of the latest news from Washington, I'm here to help. If you feel you need to change now, read: Changing my plan now!
The debate over drug pricing is really a debate over a fundamental question: How do we balance the need for affordable access to medicine today with the need to incentivize the cures of tomorrow?
There are no easy answers, but understanding the forces at play is the first step toward making informed decisions for your health and your wallet.
Have questions about how these issues might affect your specific Medicare coverage? Contact me today for a personalized consultation.